
Have you ever been left wondering why your good employee made a bad decision that resulted in an incident?
If you have, chances are your incident investigation left you a little unsatisfied. Here are 3 tips for identifying the factors that influence human reliability in your organization.
1. Approach the decision from the employee’s perspectiveRarely, if ever, do people make mistakes on purpose. Usually for the operator things are progressing exactly as expected, until they’re not. Although it is important for the investigation to understand what was supposed to have happened, the knowledge of hindsight will impede your ability to understand the thought process of the employee at the time of the incident. Avoid casting judgement on decisions made leading up to the incident and seek clarity on the thought process itself. Some questions to consider when seeking insight to your employee’s perspective might include:
- Have you done this before? What happened then? What was different about this time?
- Is there a process or procedure? Did you follow it? If not, why not?
- Have you been trained to perform this task? If so, when? How is the training different from what you were doing at the time of the incident?
- What were you tasked to do? What did your supervisor expect from you at the completion of this task?
- Did you have the equipment and information you needed to complete this task as planned? If not, what was missing?
- Where did things start to go wrong and why?
By understanding what your operators were thinking about in the moments leading up to the incident , and what cues they were using to make their decisions, you will begin to see areas within your organization that may be causing confusion or contributing in unexpected ways to the decision-making calculus of your employees.
2. Understand the system in which your employees are workingPeople do not make decisions in a vacuum. They receive and process multiple cues that inform many decisions over the course of the day. These cues could be feedback from equipment such as output pressure on a pump, or production data such as quality specifications of a chemical product. These are obvious cues from the system that in most cases will drive a predictable reaction from employees. Systems, however, are complex. Inputs and disturbances that originate several layers away from the employee will eventually make their way to the operator and may result in a reaction that is less predictable.
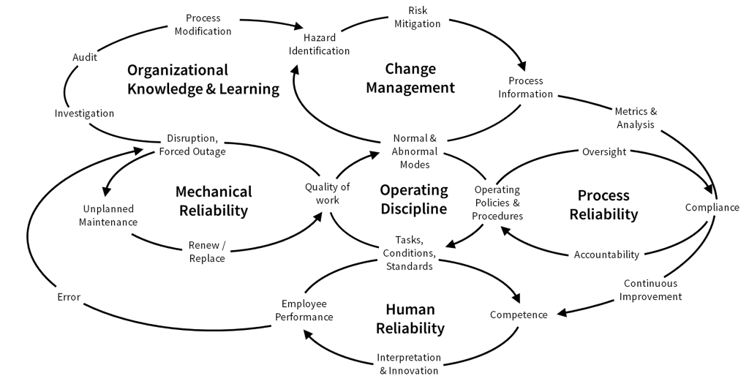
The diagram below depicts one example of the complex relationships within an organization’s operating system. A disturbance (or error) in the mechanical reliability process will eventually, if not corrected, manifest to other areas of the system. Therefore, it is important to investigate these relationships to understand how they may have influenced the decisions leading to the incident. A good technique for this is to compare what should have happened to what actually did happen and see where the differences are. For example:
- How did the plan differ from what was done?
- Were there barriers or safety measures that should have prevented this from happening? If yes, why did they fail? Were they used? Why or why not?
- Were there processes, permits, or other controls that should have prevented the incident or indicate an elevated risk level? Why did these processes not work?
- Were there alarms on the equipment? Did they work? Were they acknowledged? Why or why not? What was the operator’s reaction to the alarm? Is that a normal reaction? Is it the correct reaction?
- Was the equipment/system/process operating in a degraded mode? If yes, why and for how long? Had the degraded mode become the norm?
- How is work typically done and does the typical work pattern align with the prescribed process? If not, why not?
By understanding how disturbances in the system over time influence and reinforce certain behaviors, you can apply corrective actions to the system which will have broader impacts across the entire organization.
3. Understand the leadership, and how you and other leaders are influencing employee decisions.
Within an organization, the collective body of employees generally have a prevailing mindset about how things are done in the organization (some refer to this as the culture of the organization). This mindset drives behavior. It is influential in how people make decisions and to what standard they strive to attain. This mindset, or culture, is shaped by the organization’s leadership. For this reason, investigators must work to understand how leadership influences behavior. This can be difficult because it forces you, as a leader, to recognize the errors you have made in contributing to the events leading up to the incident. Things to consider when looking at leadership’s role in the incident include:
- What was tasked? How did that compare to what was done?
- How was the job supervised? Was there oversight? How did the supervisor practice quality control or maintain a standard of performance?
- What metrics are used to measure success? Did this influence a decision or behavior?
- How are rules, processes, and procedures enforced? Are they consistently enforced?
- What types of behaviors get rewarded? Do employees get recognized for meeting production requirements, or for following the rules? What types of decisions are you reinforcing as a leader?
- Do leaders hold themselves to a higher standard and lead by example? Do they follow processes and procedures, or do some rules not apply because they are in a position of authority?
Remember, errors occur at all levels in an organization. Investigations typically identify the errors closest to the event, but contributing errors made higher in the organization rarely get identified or corrected.
I encourage you to consider these three tips the next time you are review a root cause analysis or conducting your own investigation. To learn more about creating a more reliable and operationally resilient workforce by incorporating human factors analysis into investigations, click here.
To learn more about creating a more reliable and operationally resilient workforce by incorporating human factors analysis into investigations, click here.

 0 Comments
0 Comments
 1200 Corporate Drive, Ste 170
1200 Corporate Drive, Ste 170



